



The Phantom Pain Puzzle
Why Phantom Limbs Won't Go Away

Late one evening in July of 1797, a musket ball was fired through the air.
Europe was ablaze with the French Revolutionary Wars, and the British Royal Navy was engaged in a daring raid on the Spanish island of Tenerife. Admiral Lord Horatio Nelson led the charge.
As Nelson guided his men through the darkness, that fateful musket ball found its mark.
It struck the Admiral’s right arm, shattering bone. His men quickly rowed him back to the main ship, where his arm was surgically amputated.
In the months that followed, Nelson began to experience something bizarre.
He could still feel the arm that was no longer there.
These feelings were so vivid that he swore he could feel his nonexistent fingernails digging into his nonexistent palm.
These ghostly feelings convinced Nelson he’d stumbled upon something profound.
If a missing arm can live on after it’s gone, he declared, surely a missing whole body can, too! For Nelson, this wasn’t just a medical oddity — it was proof of life after death.
At the time, Nelson had no idea how his experience would influence the study of the fascinating but awful phenomenon we now call phantom limb pain.
So, what exactly is going on here? How can losing a body part lead to feeling pain in a limb that’s no longer there?
To find out, let’s ask three key questions:
What exactly is phantom limb pain?
What are some early hypotheses about phantom limb pain? and,
What are the latest theories?
Q1: What Exactly is Phantom Limb Pain?
Let’s start with phantom limb sensation (without the pain).
Phantom limb sensations are astonishingly common. Studies suggest that almost all amputees — upwards of 90% — will experience some form of these sensations.
Many will experience tingles, pins and needles, or even different temperatures in a limb that’s no longer there. Some folks swear they can still feel their wedding ring or wristwatch. Others report sensing their phantom limb in weird positions.
And many feel they can move their phantom limb. To these folks, moving their phantom limb still feels different from imagining moving their phantom limb.
For most of those who experience a phantom limb, their limb feels just like it did before the amputation. But some experience a phenomenon called telescoping, where the phantom limb gets shorter over time. For example, someone might feel like their hand is now attached closer to the amputation site.
Unfortunately, for many amputees, phantom sensation is not always pleasant. Phantom limb pain affects between 60% and 80% of amputees at some point after losing a limb. That’s a staggering number when you think about it.
Imagine losing a body part, only to find that your brain is convinced it’s still there — and on top of that, it causes you intense pain, which you cannot soothe with heat packs or massage.
This strange phenomenon raises all sorts of questions. How does the brain create sensations in a limb that’s no longer there? And why on earth would those sensations be painful?
We don’t have all the answers about phantom pain yet. But we do know some things.
To start painting the picture of what we know, let’s first examine some early theories.
Q2: What are Some Early Hypotheses About Phantom Limb Pain?
In last week’s article, we discussed nociceptor neurons. These neurons detect actual or potential tissue damage, sending signals to the spinal cord, where they connect with other neurons that send signals to the brain. Nociceptors are found throughout the body, including the skin. When someone has a limb amputated, let’s say their arm, these neurons are severed.
One of the first physical explanations for phantom limb pain focused on the damaged nerves at the spot where the limb was removed.
The idea is that these nerves, although they no longer connect to their original receptors in the missing limb, still generate and transmit electrical signals. These signals can occur spontaneously or be triggered by touch to the amputation site. The brain, not knowing any better, interprets these signals as coming from the phantom limb.
There’s some strong evidence to support this hypothesis.
If we press on the amputation site, the amputee will often feel pain in their phantom limb. If we record the activity of nerves at the amputation site, we find that when those nerves are highly active, the amputee is more likely to experience phantom pain.
We also know that over time, the ends of severed nerves form small swellings called neuromas. These neuromas can be hypersensitive.
But perhaps the most compelling evidence that pain sensations are triggered by the severed peripheral nerves is that if we inject local anesthesia into the amputation site, the pain often completely disappears.
These findings explain some things about phantom pain, but they don’t tell us everything. For instance, peripheral nerve activity doesn’t explain why the sensations feel like they’re coming from the missing limb and not just the amputation site. And it doesn’t account for pain. Why are phantom limbs so often painful?
As scientists continued to investigate, they soon discovered that peripheral nerve activity doesn’t tell us the whole story of phantom limb pain. To uncover more clues about this mysterious phenomenon, we need to look at what’s happening in the brain.
Q3: What are the Latest Theories?
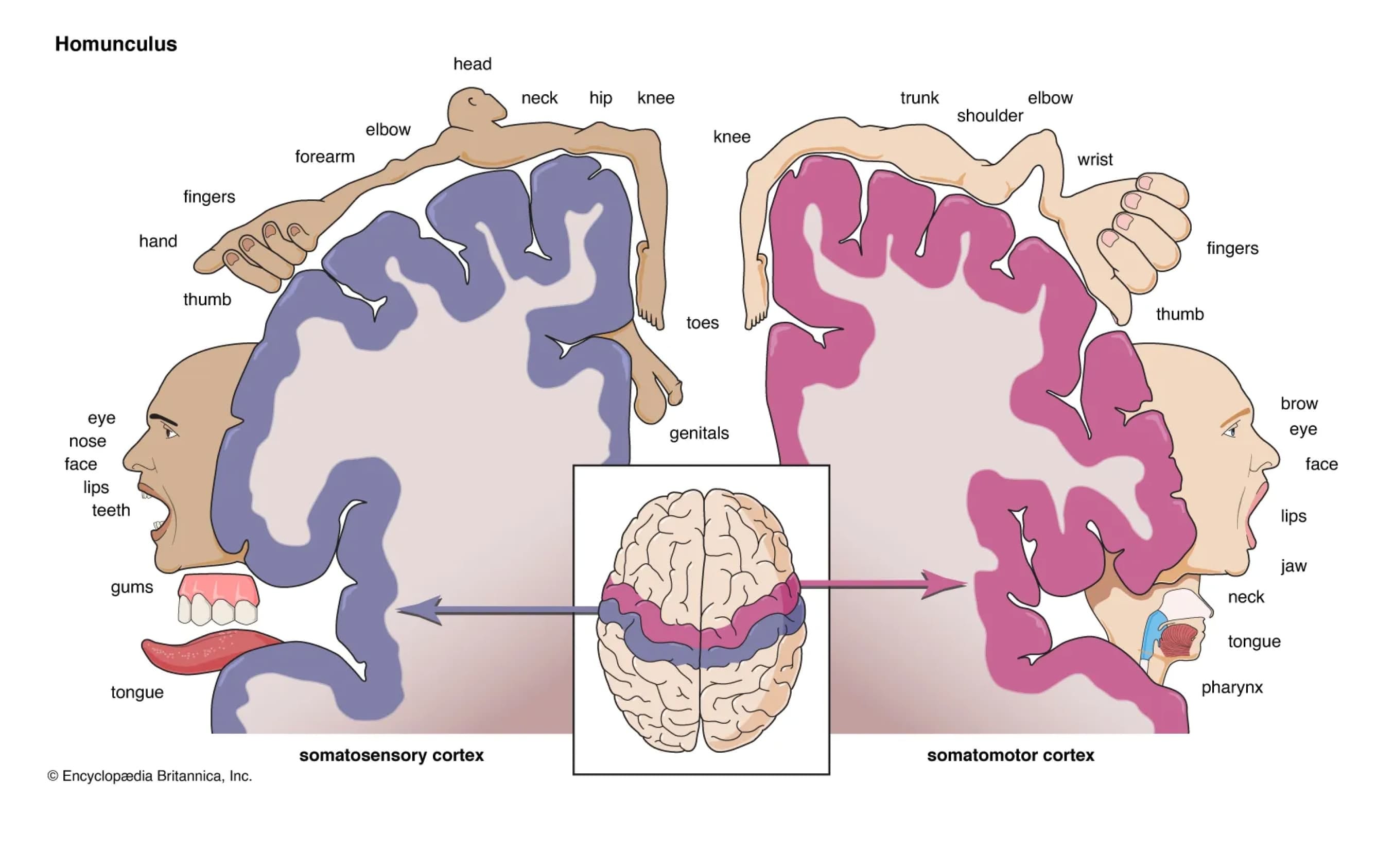
Remember the somatosensory cortex? It’s that strip of cortex that runs under your headphone band, and it is responsible for processing sensory information (purple in the image below). It acts like a map of the body that responds to sensory inputs from the body.
We have another type of map — the primary motor cortex (pink in the image below). The primary motor cortex sits just in front of the somatosensory cortex. It, too, acts like a map of the body, but instead of receiving input from the body, this area sends motor commands to the body.
Neurons in these areas are highly plastic — they change — even throughout adulthood. This ability to change is known as neuroplasticity.
Currently, the two main theories about the cause of phantom limb pain have to do with neuroplasticity in the somatosensory cortex: the maladaptive plasticity theory and the persistent representation theory. Both theories relate to how the brain changes after losing a limb, but they suggest different reasons for how phantom limbs happen and why they can cause pain.
Let’s review these two theories and then explore a new theory that might reconcile these two seemingly opposing views.
The Maladaptive Plasticity Theory
When we talk about neuroplasticity after limb loss, things can get a bit tricky, especially when referring to specific brain areas. To keep things clear, let’s narrow our discussion to arm amputation.
When someone loses an arm, the neurons in the somatosensory cortex that once responded to input from that arm suddenly have little to do. Let’s call this area of the somatosensory cortex the former sensory hand area.
In the brain, neurons that have little to do often adopt the functions of their neighbours. In the somatosensory cortex, the former sensory hand area is next to the sensory face area. So, neurons in the former sensory hand area might start acting like neurons in the sensory face area — they start responding to inputs from the face. So, the sensory face area processes inputs from the face, but now the former sensory hand area also processes inputs from the face.
When this happens, the brain’s map of the body is redrawn: the area responding to face sensations appears to expand into the former sensory hand area, essentially shrinking the former sensory hand area. This process is what neuroscientists call cortical remapping.
During the mid-90s, researchers discovered something strange: the more the former sensory hand area remaps, the more intense the phantom limb pain. In other words, the more the former sensory hand area is taken over by the face area, the worse the phantom pain tends to be. This finding sparked a series of studies suggesting that neuroplasticity in the somatosensory cortex might have maladaptive consequences.
These discoveries led to the maladaptive plasticity theory.
Since then, the maladaptive plasticity theory has been highly influential. It is the theory behind many of the popular treatments for phantom limb pain, including mirror therapy.
In mirror therapy, a mirror is placed between the amputee’s limbs, with the reflective side facing the intact limb. This creates the illusion of two intact limbs when the patient looks into the mirror. The amputee then performs symmetrical movements with both their intact limb and their phantom limb while watching the mirror. The visual feedback from the mirror shows that the missing limb is moving normally. The idea is that this visual feedback will encourage the brain to reorganise back to its pre-amputation state, reversing the maladaptive changes.
While mirror therapy has proven helpful for some patients, it’s not universally effective. In fact, for some individuals, mirror therapy can even increase pain.
Since the mid-90s, the maladaptive plasticity theory has been the prevailing explanation for phantom limb pain. However, it doesn’t provide all the answers. For instance, it doesn’t explain why some amputees experience phantom pain immediately after amputation before remapping has had time to occur. And it doesn’t explain why these experiences are painful. Why would remapping produce pain?
These unanswered questions suggest that the maladaptive plasticity theory may not be the whole story. What else might be going on with phantom limb pain?
The Persistent Representation Theory
In 2013, a paper published in Nature Communications challenged the maladaptive plasticity theory and proposed a new theory: the persistent representation theory.
This study was similar to the original study from the ‘90s, but instead of stimulating different parts of the amputation site, the researchers asked participants to move their phantom limbs.
The results were surprising. The researchers found that the more someone experiences phantom pain, the more their former sensory hand area maintained its original mapping.
This finding seems contrary to what the maladaptive plasticity theory would predict.
Because the maladaptive plasticity theory suggests neighbouring areas take over the former sensory hand area, we might expect that after remapping, the new sensory hand area would be smaller and, therefore, show less activation, not more.
At first glance, the maladaptive plasticity theory and the persistent representation theory seem to contradict each other: one suggests that phantom pain is linked to the loss of limb representation, while the other associates it with the persistence of that representation.
So…
How do we reconcile the evidence supporting these two theories?
The key to understanding this puzzle might lie in how these studies were done.
For the most part, the two theories are supported by different types of studies. The maladaptive plasticity theory is based on studies where researchers passively stimulated the amputation site. The persistent representation theory, on the other hand, comes from studies where participants actively moved their phantom limbs.
This difference in methods is crucial.
The somatosensory cortex receives different types of inputs in these two situations. What comes into the somatosensory cortex during passive stimulation is quite different from what happens during attempted movement.
If you’re a regular reader of this newsletter, you might already know where this is going.
In the article Can We Have a Mind Without a Body, we explored the idea of an efference copy. And it turns out that efference copies might be important here too.
If you need a recap of efference copies, here’s an extract from that article :
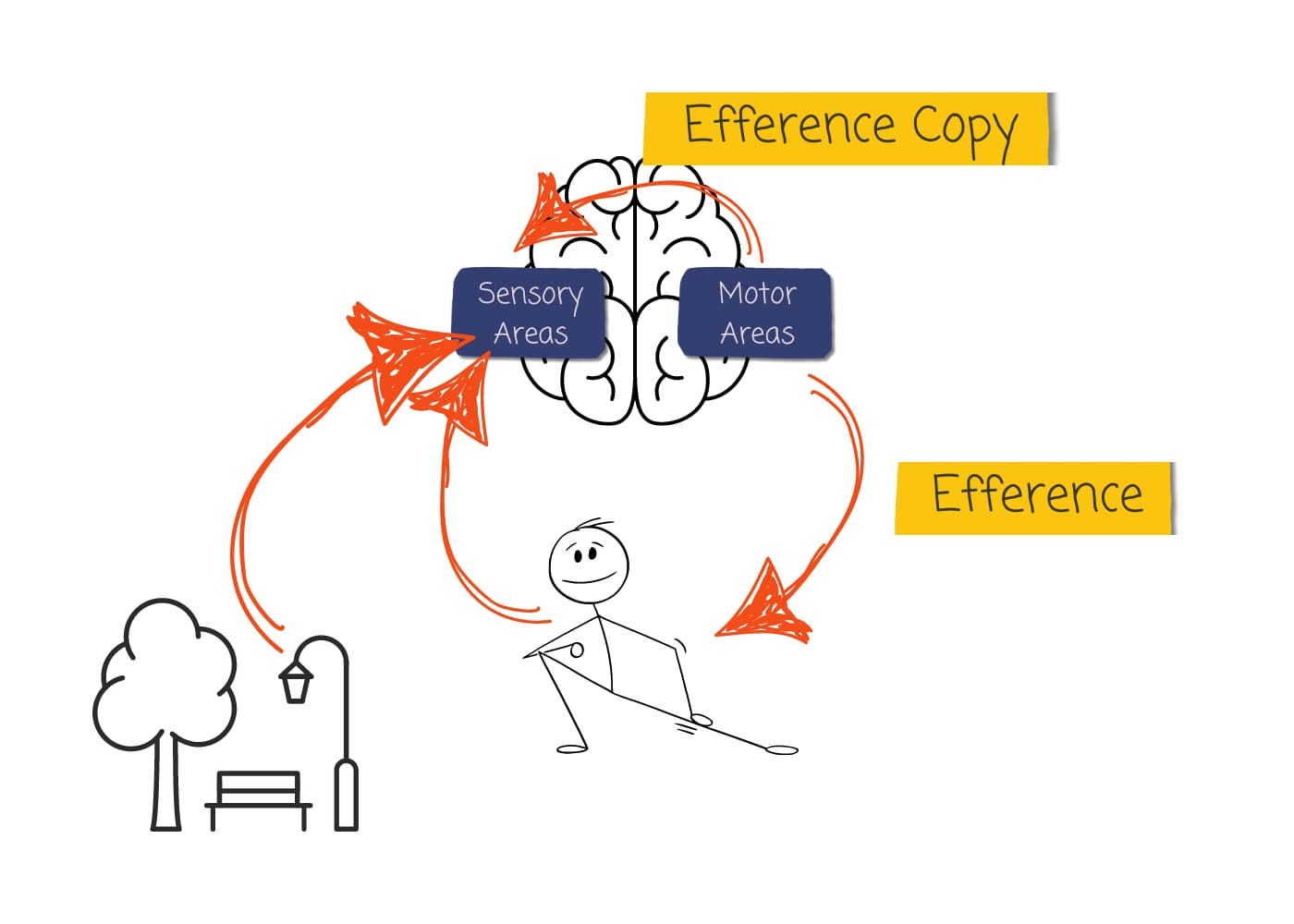
In neuroscience, efference refers to signals sent from the brain to the body (like motor commands), while afference refers to signals sent from the body to the brain (like sensory information). Just remember E for Exiting the brain and A for Arriving.
As the name suggests, efference copy is a copy of the efferent signal produced by the motor areas.
When your brain sends a command to move a part of your body, it doesn’t exclusively send the command to the body; it also sends a copy of this command to other parts of the brain, including the sensory areas.
The efference copy serves as a prediction of the sensory consequences of our actions. In other words, the efference copy is compared with the actual sensory input it gets from the action the body makes.
So, in studies where the researchers passively stimulate the amputation site, the somatosensory cortex receives input from the body (sensory receptors), but it doesn’t receive an efference copy. This is because when passively stimulated, the person isn’t planning or executing a movement, so the motor cortex isn’t sending out motor commands or efference copies.
But when an amputee attempts to move their phantom limb, the motor cortex sends out commands to move the limb, and it also sends an efference copy of these commands to other parts of the brain, including the somatosensory cortex. The motor cortex does this regardless of whether the limb is physically present.
So when someone tries to move their phantom limb, their former sensory hand area receives a much richer mix of signals. It gets efference copies from the motor cortex and sensory input from the amputation site. But it might also get input from other areas, like the pain suppression pathway, which we talked about last week.
In other words, the former sensory hand area would get very different input during movement compared to passive touch. And because different inputs lead to different neurons being activated, we see different brain patterns in the two types of studies.
This raises an interesting question: could a mismatch between brain activation explain pain?
To answer this question, we need to briefly discuss a prominent scientific theory of how the brain works:
The Predictive Coding Theory
The predictive coding theory suggests that perception — including our perception of pain — results from a continuous interaction between what the brain expects and the actual sensory input it gets. In other words, the brain is constantly making predictions and updating those predictions based on the sensory information it receives from the body and the environment. When what the brain expects doesn’t match what it actually senses, it creates a prediction error.
The efference copy provides the prediction — the brain’s best guess about what sensory inputs to expect from the planned movement.
But with phantom limb pain, it doesn’t receive what it expects. The former sensory hand area either receives no input or, because of cortical remapping, receives unexpected input (sensory inputs from the face, for example). This mismatch between expected and actual sensory input creates a prediction error.
Pain might be our brain’s way of signalling this error. It’s telling us something is wrong with the brain’s model of the body.
Predictive coding theory could explain why treatments like mirror therapy can be effective for some but not others. Mirror therapy may work by providing visual feedback that matches the brain’s predictions, reducing the prediction error. But in cases where the visual feedback doesn’t match the brain’s expectations (such as in patients with telescoping or patients who feel their limb is in a strange position), it might not be effective or could even exacerbate the pain.
Predictive coding theory might also explain how both the maladaptive plasticity and persistent representation theories could be right. It suggests that both contribute to phantom limb pain, just in different ways.
Neurons need consistent input to maintain their representation. Different input often results in remapping.
So, when the amputation site is passively stimulated, the former sensory hand area gets different inputs from what it would have gotten before the amputation. The different input results in remapping.
But when the brain tries to move the limb, the former sensory hand area gets inputs similar to what it would have gotten before the amputation — both from the efference copy and, ironically, from the pain itself. The very experience of pain in the phantom hand might provide the input that helps maintain the representation in the former sensory hand area.
This creates a vicious cycle: the pain helps maintain the representation, but passive input from the missing limb causes remapping, and the mismatch between the preserved representation and the remapping leads to more pain.
We still don’t have all the answers when it comes to phantom limb pain. Most of the research has focused on the somatosensory cortex, but we know that multiple brain areas are involved in pain. There’s much more work to be done.
This article ends our series on pain (although we will talk more about pain next year when we talk about robots).
The last couple of articles have been heavy on neuroscience. So, next week, let’s jump back into the philosophy of mind. We’ll start a new mini-series on experience — what does experience teach us, and what can we know without experiencing?

Thank you.
I want to take a small moment to thank the lovely folks who have reached out to say hello and joined the conversation here on Substack.
If you’d like to do that, too, you can leave a comment, email me, or send me a direct message. I’d love to hear from you. If reaching out is not your thing, I completely understand. Of course, liking the article and subscribing to the newsletter also help the newsletter grow.
If you would like to support my work in more tangible ways, you can do that in two ways:
You can become a paid subscriber
or you can support my coffee addiction through the “buy me a coffee” platform.
I want to personally thank those of you who have decided to financially support my work. Your support means the world to me. It’s supporters like you who make my work possible. So thank you.
Great article on phantom pain. Always enjoy your musings and discussions.
Thx.
Respectfully.
I enjoy neuroscience articles! But I know from my own blog that philosophy ones tend to be more popular. Anyway, I didn't realize anesthetizing the amputation site was effective. Although the fact that that didn't end the investigation seems to show that no one answer will probably resolve it.
I think predictive coding has a lot of promise, so it's kind of exciting to see it possibly having some use in clinical scenarios. I don't see it as a complete alternative to other scientific theories like global workspace, attention schema, or higher order theories. I think they're all modeling different aspects of the overall reality.
But I like predictive coding because it seems to provide an explanation for the first glimmers of cognition in those early Cambrian or pre-Cambrian animals. We get stimulus-response from diffuse nerve nets and spinal cords, but prediction explains what the earliest additions to those automatic responses would have added, and how cognition overall began to evolve.
Interesting article, as always Suzi!